


 Shoulder Conditions & Treatment Options
Shoulder Conditions & Treatment Options
At Joint Preservation Institute, we take care of many patients who have shoulder pain. Conditions that we commonly see include frozen shoulder, shoulder impingement, labrum injuries, biceps tendon injuries, rotator cuff tears, and shoulder arthritis. We also take care of many traumatic injuries including dislocated shoulders, tendon tears around the shoulder, and shoulder separations.
A brief review of the anatomy of the shoulder reveals a ball and socket joint that is relatively shallow compared to that of the hip. The shallow shoulder socket allows us to have a wide range of motion. Additionally, about one third of the shoulder range of motion occurs between the shoulder blade and the chest wall, called the scapulothoracic joint. The shoulder is stabilized by a thick connective tissue called the capsule as well as the rotator cuff muscles. The rotator cuff muscles are a group of 4 muscles with important function in the movement of the shoulder joint. These muscles have relatively limited blood supply and are often very prone to tearing either from traumatic events or from overuse and by chronic impingement between bony structures of the shoulder.
Bony Anatomy of the Shoulder Joint

Muscular and Soft Tissue Anatomy of the Shoulder Joint

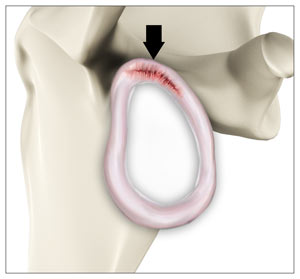
Another structure that is important for the stability of the shoulder is the shoulder labrum which acts both to deepen the shoulder joint and as a bumper and suction cup to protect and stabilize the shoulder. It is highly innervated and can often be torn either from a shoulder dislocation or from a violent pull of the long head of the biceps tendon which attaches to the upper part of the labrum.
Standard x-rays are usually indicated for most shoulder injuries but often an MRI of the shoulder is necessary. The MRI provides great detail about the state of the multiple structures the shoulder including bone, muscles, tendons, ligaments, labrum, and the two main joints of the shoulder, the glenohumeral joint and the acromioclavicular joint.
Frozen shoulder is a very common condition which we see and can be effectively treated with physical therapy. In some select cases, frozen shoulder may need to be treated with an arthroscopic procedure. It is critical to resume physical therapy after the procedure to maintain the range of motion.
Rotator cuff tears, particularly if they are partial-thickness can also be treated with physical therapy and sometimes injections. If there are full thickness tears, most frequently occur in the supraspinatus muscle can also occur in the infraspinatus or subscapularis.
Rotator Cuff Tears

Full thickness rotator cuff tears usually require surgical repair. This can be done with an all arthroscopic technique. Dr Jamali has extensive experience with all levels of arthroscopic rotator cuff repair. If the tears are long-standing and chronic, the tendon of the rotator cuff sometimes is scarred and shortened and cannot be repaired. In these cases a specialized procedure called a superior capsular reconstruction may be required to augment the native rotator cuff.
Labrum Tears
Labrum tears often occur from a traumatic event or from overuse. They can be treated without surgery if they respond to physical therapy and injections. Labrum tears can occur either as a result of the pull of the biceps tendon on the superior labrum or secondary to dislocations which are typically seen in the anterior bottom part of the labrum. The labrum tears that are associated with a dislocation of the shoulder are commonly called a Bankart lesion

Otherwise, they need arthroscopic surgery. The arthroscopic surgery for the labrum can entail either a primary repair or a combination of labral repair or debridement and a biceps procedure if the labrum involves the attachment point of the biceps.
Most types of labrum tears can be treated non-operatively initially. If they become persistently painful or are associated with recurrent episodes of dislocations or instability of the shoulder then a surgical repair is usually required. Instability is when the shoulder feels like it is going to slide out of the socket with routine activities. Most repairs of the labrum can be done arthroscopically and have excellent outcomes due to the minimally invasive nature of the surgery with very little damage to the surrounding tissue and the ability to eliminate pain very quickly after the surgery.
Repairing the labrum alone especially in older patients is not been as effective as detaching the biceps and fixing it elsewhere down the bone of humerus. That procedure is called the biceps tenodesis (see below).
Biceps Injuries in the Shoulder
The biceps muscle is present on the front side of your upper arm and functions to help you bend and rotate your arm. The biceps muscle has two attachments at the shoulder. The long head of the biceps is the one that often gets injured in shoulders as a result of trauma or degenerative wearing out. It attached to the top of the labrum and often is a factor in causing one kind of labrum tear called a superior labrum tear discussed above.
A Biceps tendon rupture can either be partial, where it does not completely tear the tendon, or complete, where the biceps tendon completely splits in two and is torn away either from the top of the labrum or near its attachment there.
The Biceps tendon can tear at the shoulder joint or elbow joint. Most biceps tendon ruptures occur at the shoulder and is referred to as proximal biceps tendon rupture and involve the long head of the biceps. The reason for its common tearing is that the long head of the biceps goes into a tunnel where it can be damaged and then eventually attaches to the shoulder labrum. It can be injured in the tunnel over time and with activity or by an injury that leads to sudden pull on the tendon.
The most common symptoms of a biceps tendon rupture include a sudden, sharp pain in the upper arm, audible popping sound at the time of injury, a bulge above the elbow (Popeye sign), and/or bruising to the upper arm.
Arthritis of the Shoulder
Arthritis of the shoulder can sometimes be treated with injections and physical therapy.

Fortunately since the shoulder is a nonweightbearing joint to the arthritis is relatively well-tolerated. More advanced cases shoulder replacement surgery may be necessary.
Total Shoulder Replacement
Shoulder replacements are divided into standard or anatomic shoulder replacements which are done when the rotator cuff is relatively healthy and reverse shoulder replacements which are done with the rotator cuff is very damaged and not able to be repaired.
Both of these procedures have excellent outcomes. Our preference is to perform the anatomic replacement of the rotator cuff is healthy.
Anatomic Total Shoulder Replacement
Anatomic total shoulder replacement (shown below) is performed most often for the diagnosis of shoulder arthritis. This procedure is a resurfacing of the joint by putting a new ball where the native ball of the humerus is located (the humeral head), and a new socket on the native shoulder socket, called the glenoid. It depends on the function of the rotator cuff to stabilize and move the shoulder. Therefore, we often obtain an MRI of the shoulder prior to performing this type of shoulder replacement to see the health of the rotator cuff muscles.

Reverse Total Shoulder Replacement
The reverse total shoulder replacement (shown below) gets its name as it reverses the position of the ball and socket of the shoulder. An artificial ball is placed on the glenoid, the shoulder socket and an artificial socket is placed on the upper arm bone which normally is the ball of the native shoulder. This is done in order to improve the biomechanics of the shoulder in the setting of severe damage to the rotator cuff. This biomechanical improvement allows the shoulder to work with the reverse shoulder replacement even in the complete absence of the rotator cuff from trauma or from long standing tears.
